There has been a large focus in the Physiotherapy and personal training world over the past decade by many presenters and authors on making rehab and training “functional” and only using multijoint movements for specific problems. Squats or leg press are advocated to load a patellar tendinopathy, shoulder press for rotator cuff related shoulder pain and single leg activities eg single leg squats for running injuries. In reality are “functional” exercises important? Should we base our early stage rehabilitation on multijoint “functional” exercises, movements that replicate your patients sport or activity, or should these exercises be left to the later stages of rehabilitation?
The principles of specificity utilise the SAID principle - Specific adaptation to an imposed demand, meaning the body will have an improvement only in movements, muscles and ranges trained. For example, if you want to improve squatting strength, we need to train a squat, or if you want to improve your running speed you need to train speed into your running program. Other “non-functional” or non-specific exercises will have no effect on squatting or running. In reality, how true is this?
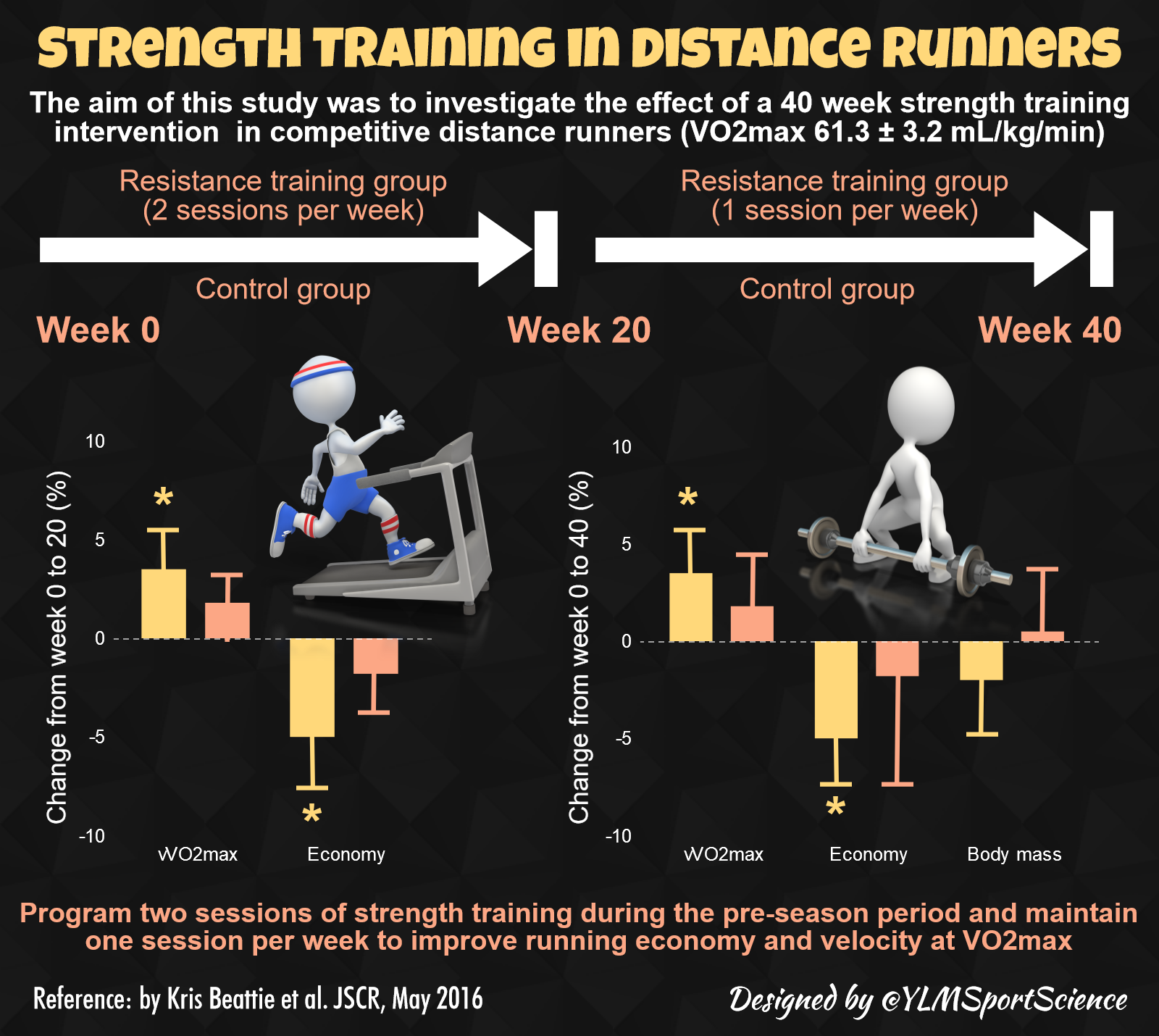
Interestingly, an abundance of studies (see below) demonstrate increased running speed and efficiency with strength training using heavy weights in squats, deadlifts and other exercises that are non-specific to running, in a repetition range of 6–10 reps.
Where does specificity of response fit into this, how does distance running relate to heavy weights? How could running efficiency and speed in a 20 minute event be increased with heavy weights performed in sets lasting only 30 seconds? These exercises aren’t even single leg exercises or plyometric in any way. This doesn’t fit the SAID principle at all, and raises questions regarding whether exercise response is really as specific as we once thought it was.
If specificity is in question, do we need to make our rehabilitation exercises look like the movements the patient needs to perform, especially in the early stages. In the later stages of rehabilitation, performing multijoint exercises to increase overall strength and control and prepare your patient for return to sport is positive, but how necessary is it in the early stages to make exercises functional?
In many cases functional or multijoint exercises in the early stages may detract from your results rather than aid your patients recovery. If your patient has a patellar tendinopathy, performing only functional and multijoint movements such as squats or leg press may only minimally improve the load capacity of the patellar tendon, and result in little or no improvement in symptoms. Surely if your patient is using heavy weights in their squats the patellar tendon will increase the load capacity?
Unfortunately this is not always the case, as a common substitution for loading the quadriceps and patellar tendon is to increase activity in the gluteals or hamstrings (1). Without providing adequate stimulus and load to the quadriceps and patellar tendon, the load tolerance of the patellar tendon will not increase enough to cope with daily or sporting requirements.
Isolation exercises such as leg extension or the spanish squat may help initially to load the quadriceps and patellar tendon adequately to create adaptation, especially when used in a range that is less likely to compress or irritate the tendon eg 30 to 60 degrees knee flexion.
When symptoms are settling and load capacity of the tendon has improved, larger multijoint or “functional exercises” can be incorporated to increase overall load capacity and strength of the quadriceps and patellar tendon, followed by energy storage activities eg A-skips, plyometrics.
If you only utilise functional multijoint exercises you may miss the essential components of increasing load capacity in the area you need to target, whether that is the patellar tendon, rotator cuff, hamstrings or any other areas. Of course there are many other biopsychosocial aspects to pain, including the neurotags and pain association with different movements, and your patients may sometimes need some help to desensitise these movements etc, but for the sake of this blogpost, let’s focus on the physiological aspects.
So don’t be afraid to utilise isolation style exercises even thought they aren’t “functional” or specific, especially in the early stages of your rehabilitation.
When do you use isolation or functional exercises? Let me know on Twitter
Related resources
Physio Edge podcast 023 - Lower limb tendinopathies with Dr Peter Malliaras
References
{kind=link}
Transcription
Hi I’m David Pope and welcome to this weeks five-minute physio tip on the myths of specificity and functional exercises. So the question is, do you need to be really specific to the person’s function? If the patient has pain during a functional task, do you need to retrain that functional task?
For instance squatting, do you need to retrain their squat or their leg press if that’s what really important to them and they’ve got pain during it. Or are you best performing other tasks?
I’m sure at uni you learnt the principles of specificity, that you had a specific adaptation to a specific demand. So for instance if you were training your biceps and you strengthen them between 80–120 degree of elbow flexion, that you got stronger in that range but not in other ranges or movements related to your biceps. Makes sense, but, how true is it?
Let’s take for example leg press. Your patient has got patellar tendinopathy, with anterior knee pain in the patellar tendon while they’re performing a leg-press and they really want to get back to it. So can we just get them doing squats or leg-presses as their patellar tendon loading program or do we need something else that’s unrelated to the squats or leg-presses that they want to do.
There was a really interesting study that compared one legged leg-press in patients with patellar tendinopathy and looked at their strength. And what they found was that their strength in the leg-press in their affected side was just as strong, if not stronger in their affects side just as much as their unaffected side. But when they compared their quadriceps strength with isokinetic knee dynamometry they found that their knee extension strength was decreased. So their quadriceps didn’t have the strength, the patellar tendon didn’t have the load capacity it would have despite having great strength in their leg-press. So how does that work?
You can imagine if you’re performing a leg-press and you’re pushing 100kgs. You can either achieve this through loading your quadriceps a certain amount, or you can tie in other muscles so for instance your glutes, calves, hamstrings and then take up the remainder with your quadriceps. So you can get around it, you can work around holes in your kinetic chain by incorporating muscles to achieve the same desired output, for instance 100kg leg-press.
If you just perform squats or leg-press as your functional retraining for a patellar tendinopathy are you really going to load that patellar tendon enough to increase it’s load capacity? No. Because you’re not actually loading the quadriceps enough to have a stimulating effect. So in this case, you really want to step away from your specific functional exercises, your squats and your leg-presses. Take it back to a more isolated exercise for instance starting with isometric knee extension and then getting the load capacity of the patellar tendon, increasing that strength and then after you’ve built that strength up then you can incorporate it back into those sort of functional exercises.
You then have the load capacity there you can actually incorporate the quadriceps and get that load onto the quadriceps and the patellar tendon. So that’s a really good example of when you need to be non-specific, but then bring that specificity and functional training back in later to tie in that whole kinetic chain.
So when you’re looking at all your exercises and trying to decide do I need to make this really functional if it’s a compound movement, for instance they’re having pain with pushups or throwing. Do we need to retrain that specific task?
Often times you can address the specific components related to it early in the treatment. Does it need to be specific and functional to their throwing for instance but you can break it up all into components, tie it all together later and it works really well. It lets you address each individual component.
So that’s all for this weeks 5 minute physio tip, hope you’ve enjoy it. If you’ve found us anywhere else but our blog at clinicaledge.co head on over check out all the podcasts, the blog posts and videos we’ve got for you there and have a great week.